Suffering from Knee Pain?
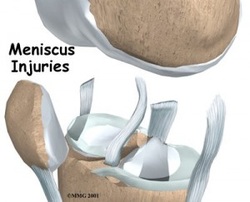
The knee is not only the largest joint in the body, it is in fact consist of two joints. The larger of the two is the joint between the thighbone and the larger of the lower leg bones. The kneecap or patella is a bone within the tendon of the quadriceps muscle. The patella forms a joint with the femur that shares the same capsule as the joint between the femur and tibia. The latter joint has two half-moon-shaped pieces of cartilage called menisci that both guide the bones as they move and take about 60 percent of the weight going through the knee. In addition, there are a large number of muscles, ligaments, and tendons acting to move or stabilize the knee. Pain may arise from all these structures either singly or in combination. Some causes of knee pain are obvious while others may require expert examination and special investigations to diagnose. Some may arise outside the knee. A well-known source of pain referred to the knee is arthritis. Knee pain can hinder a person from walking properly and prolong suffering, action should be taken as soon as possible to avoid further damage to the affected tissues and bones. Below are the list of problems:
|
Anterior Cruciate Ligament (ACL)
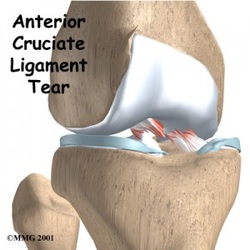
What is Anterior Cruciate Ligament (ACL) Injury? The anterior cruciate ligament, or ACL, is one of four major knee ligaments. The ACL is critical to knee stability, and people who injure their ACL often complain of symptoms of their knee giving-out from under them. Therefore, many patients who sustain an ACL tear opt to have surgical treatment of this injury.
What are the symptoms? The diagnosis of an ACL tear is made by several methods. Patients who have an ACL tear often have sustained an injury to the knee. The injury is often sports-related. They may have felt a “pop” in their knee, and the knee usually gives-out from under them.
ACL tears cause knee swelling and pain. On examination, your doctor can look for signs of instability of the knee. These special tests place stress on the ACL, and can detect a torn ligament.
An MRI may also be used to determine if the ligament is torn, and also to look for signs of any associated injuries in the knee.
Is ACL surgery necessary? ACL tears do not necessarily require surgery. There are several important factors to consider before undergoing ACL surgery. First, do you regularly perform activities that normally require a functional ACL? Second, do you experience knee instability? If you don’t do sports that require an ACL, and you don’t have an unstable knee, then you may not need ACL surgery.
There is also a debate about how to treat a partial ACL tear. If the ACL is not completely torn, then ACL reconstruction surgery may not be necessary.
Many patients with an ACL tear start to feel better within a few weeks of the injury. These individuals may feel as though their knee is normal again, but the problems with instability may persist.
Surgery of an ACL tear The usual surgery for an ACL tear is called an ACL reconstruction. A repair of the ligament is rarely a possibility, and thus the ligament is reconstructed using another tendon or ligament to substitute for the torn ligament.
There are several options for how to perform ACL surgery. The most significant choice is the type of graft used to reconstruct the torn ACL. There are also variations in the procedure, such as the new ‘double-bundle’ ACL reconstruction.
Risks of ACL surgery include infection, persistent instability and pain, stiffness, and difficulty returning to your previous level of activity. The good news is that better than 90% of patients have no complications with ACL surgery.
What are the symptoms? The diagnosis of an ACL tear is made by several methods. Patients who have an ACL tear often have sustained an injury to the knee. The injury is often sports-related. They may have felt a “pop” in their knee, and the knee usually gives-out from under them.
ACL tears cause knee swelling and pain. On examination, your doctor can look for signs of instability of the knee. These special tests place stress on the ACL, and can detect a torn ligament.
An MRI may also be used to determine if the ligament is torn, and also to look for signs of any associated injuries in the knee.
Is ACL surgery necessary? ACL tears do not necessarily require surgery. There are several important factors to consider before undergoing ACL surgery. First, do you regularly perform activities that normally require a functional ACL? Second, do you experience knee instability? If you don’t do sports that require an ACL, and you don’t have an unstable knee, then you may not need ACL surgery.
There is also a debate about how to treat a partial ACL tear. If the ACL is not completely torn, then ACL reconstruction surgery may not be necessary.
Many patients with an ACL tear start to feel better within a few weeks of the injury. These individuals may feel as though their knee is normal again, but the problems with instability may persist.
Surgery of an ACL tear The usual surgery for an ACL tear is called an ACL reconstruction. A repair of the ligament is rarely a possibility, and thus the ligament is reconstructed using another tendon or ligament to substitute for the torn ligament.
There are several options for how to perform ACL surgery. The most significant choice is the type of graft used to reconstruct the torn ACL. There are also variations in the procedure, such as the new ‘double-bundle’ ACL reconstruction.
Risks of ACL surgery include infection, persistent instability and pain, stiffness, and difficulty returning to your previous level of activity. The good news is that better than 90% of patients have no complications with ACL surgery.
|
Posterior Cruciate Ligament (PCL)
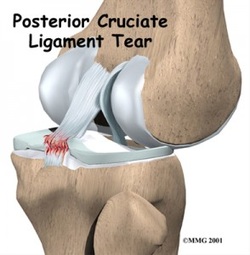
What is Posterior Cruciate Ligament (PCL) Injury? The posterior cruciate ligament, or PCL, is one of four ligaments important to the stability of the knee joint. The anterior cruciate ligament, or ACL, sits just in front of the PCL. The ACL is much better known, in part because injuries to the ACL are much more commonly diagnosed than injuries to the PCL. Interestingly, it is thought that PCL injuries account for about 20 of knee ligament injuries, however, the PCL is seldom talked about because these injuries are often left undiagnosed.
The PCL is the ligament that prevents the tibia (shin bone) from sliding too far backwards. Along with the ACL which keeps the tibia from sliding too far forward, the PCL helps to maintain the tibia in position below the femur (thigh bone).
What are the symptoms? The most common symptoms of a PCL tear are quite similar to the symptoms of an ACL tear. Knee pain, swelling, and decreased motion are common with both injuries. Patients may have a sensation that their knee “popped” or gave out. Problems with knee instability in the weeks and months following PCL injury are not as common as instability following an ACL tear. When patients have instability after a PCL injury they usually state that they can’t “trust” their knee, or that it feels as though the knee may give out. If this complaint of instability is a problem after a PCL injury, it may be an indicator that surgery is recommended.
How is PCL diagnosed? Part of the diagnosis of a PCL tear is made by knowing how the injury happened. Knowing the story of the injury (for example, the position of the leg and the action taking place) will help in making the diagnosis. Specific maneuvers can test the function of the PCL. The most reliable is the posterior drawer test. With the knee bent, your doctor will push the tibia backwards; this stresses the PCL. If the PCL is deficient or torn, the tibia will slide too far backwards, and indicate an injury to the PCL.
X-rays and MRIs are also helpful in clarifying the diagnosis and detecting any other structures of the knee that may be injured. It is common to find other ligament injuries or cartilage damage when a PCL tear is found.
PCL tears are graded by the severity of injury, grade I through grade III. The grade is determined by the extent of laxity measured during your examination. In general, grading of the injury corresponds to the following:
Surgical reconstruction of the PCL is controversial, and usually only recommended for grade III PCL tears. Because of the technical difficulty of the surgery, some orthopedic surgeons do not see the benefit of PCL reconstruction. Others, however, believe PCL reconstruction can lead to improved knee stability and lower the likelihood of problems down the road.
Surgical PCL reconstruction is difficult in part because of the position of the PCL in the knee. Trying to place a new PCL graft in this position is difficult, and over time these grafts are notorious for stretching out and becoming less functional. Generally, surgical PCL reconstruction is reserved for patients who have injured several major knee ligaments, or for those who cannot do their usual activities because of persistent knee instability.
The PCL is the ligament that prevents the tibia (shin bone) from sliding too far backwards. Along with the ACL which keeps the tibia from sliding too far forward, the PCL helps to maintain the tibia in position below the femur (thigh bone).
What are the symptoms? The most common symptoms of a PCL tear are quite similar to the symptoms of an ACL tear. Knee pain, swelling, and decreased motion are common with both injuries. Patients may have a sensation that their knee “popped” or gave out. Problems with knee instability in the weeks and months following PCL injury are not as common as instability following an ACL tear. When patients have instability after a PCL injury they usually state that they can’t “trust” their knee, or that it feels as though the knee may give out. If this complaint of instability is a problem after a PCL injury, it may be an indicator that surgery is recommended.
How is PCL diagnosed? Part of the diagnosis of a PCL tear is made by knowing how the injury happened. Knowing the story of the injury (for example, the position of the leg and the action taking place) will help in making the diagnosis. Specific maneuvers can test the function of the PCL. The most reliable is the posterior drawer test. With the knee bent, your doctor will push the tibia backwards; this stresses the PCL. If the PCL is deficient or torn, the tibia will slide too far backwards, and indicate an injury to the PCL.
X-rays and MRIs are also helpful in clarifying the diagnosis and detecting any other structures of the knee that may be injured. It is common to find other ligament injuries or cartilage damage when a PCL tear is found.
PCL tears are graded by the severity of injury, grade I through grade III. The grade is determined by the extent of laxity measured during your examination. In general, grading of the injury corresponds to the following:
- Grade I:Partial tears of the PCL.
- Grade II: Isolated, complete tear to the PCL.
- Grade III: Tear of the PCL with other associated ligament injury.
Surgical reconstruction of the PCL is controversial, and usually only recommended for grade III PCL tears. Because of the technical difficulty of the surgery, some orthopedic surgeons do not see the benefit of PCL reconstruction. Others, however, believe PCL reconstruction can lead to improved knee stability and lower the likelihood of problems down the road.
Surgical PCL reconstruction is difficult in part because of the position of the PCL in the knee. Trying to place a new PCL graft in this position is difficult, and over time these grafts are notorious for stretching out and becoming less functional. Generally, surgical PCL reconstruction is reserved for patients who have injured several major knee ligaments, or for those who cannot do their usual activities because of persistent knee instability.
Medial Collateral Ligament (MCL)
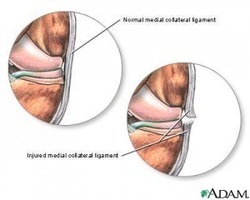
What is Medial Collateral Ligament (MCL) Injury? The medial collateral ligament (MCL) is one of four ligaments that are critical to the stability of the knee joint. A ligament is made of tough fibrous material and functions to control excessive motion by limiting joint mobility. The four major stabilizing ligaments of the knee are the anterior and posterior cruciate ligaments (ACL and PCL, respectively), and the medial and lateral collateral ligaments (MCL and LCL, respectively).
The MCL spans the distance from the end of the femur (thigh bone) to the top of the tibia (shin bone) and is on the inside of the knee joint. The MCL resists widening of the inside of the joint, or prevents “opening-up” of the knee.
Because the MCL resists widening of the inside of the knee joint, the ligament is usually injured when the outside of the knee joint is struck. This force causes the outside of the knee to buckle, and the inside to widen. When the MCL is stretched too far, it is susceptible to tearing and injury. This is the injury seen by the action of “clipping” in a football game.
An injury to the MCL may occur as an isolated injury, or it may be part of a complex injury to the knee. Other ligaments, most commonly the ACL, or the meniscus, may be torn along with a MCL injury.
What are the symptoms? The most common symptom following an MCL injury is pain directly over the ligament. Swelling over the torn ligament may appear, and bruising and generalized joint swelling are common 1 to 2 days after the injury. In more severe injuries, patients may complain that the knee feels unstable, or feel as though their knee may ‘give out’ or buckle.
Symptoms of a MCL injury tend to correlate with the extent of the injury. MCL injuries are usually graded on a scale of I to III.
The MCL spans the distance from the end of the femur (thigh bone) to the top of the tibia (shin bone) and is on the inside of the knee joint. The MCL resists widening of the inside of the joint, or prevents “opening-up” of the knee.
Because the MCL resists widening of the inside of the knee joint, the ligament is usually injured when the outside of the knee joint is struck. This force causes the outside of the knee to buckle, and the inside to widen. When the MCL is stretched too far, it is susceptible to tearing and injury. This is the injury seen by the action of “clipping” in a football game.
An injury to the MCL may occur as an isolated injury, or it may be part of a complex injury to the knee. Other ligaments, most commonly the ACL, or the meniscus, may be torn along with a MCL injury.
What are the symptoms? The most common symptom following an MCL injury is pain directly over the ligament. Swelling over the torn ligament may appear, and bruising and generalized joint swelling are common 1 to 2 days after the injury. In more severe injuries, patients may complain that the knee feels unstable, or feel as though their knee may ‘give out’ or buckle.
Symptoms of a MCL injury tend to correlate with the extent of the injury. MCL injuries are usually graded on a scale of I to III.
- Grade I MCL Tear
This is an incomplete tear of the MCL. The tendon is still in continuity, and the symptoms are usually minimal. Patients usually complain of pain with pressure on the MCL, and may be able to return to their sport very quickly. Most athletes miss 1-2 weeks of play. - Grade II MCL Tear
Grade II injuries are also considered incomplete tears of the MCL. These patients may complain of instability when attempting to cut or pivot. The pain and swelling is more significant, and usually a period of 3-4 weeks of rest is necessary. - Grade III MCL Tear
A grade III injury is a complete tear of the MCL. Patients have significant pain and swelling, and often have difficulty bending the knee. Instability, or giving out, is a common finding with grade III MCL tears. A knee brace or a knee immobilizer is usually needed for comfort, and healing may take 6 weeks or longer.
Lateral Collateral Ligament (LCL)
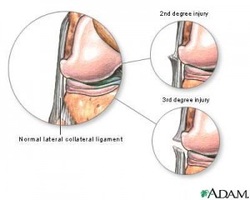
What is Lateral Collateral Ligament(LCL) Injury ? The lateral collateral ligament is the main supporting structure on the outside of the knee. It provides stability to the joint when the knee is pushed outward. A lateral collateral ligament (LCL) injury is usually a mild problem. There are three degrees of ligament injuries. A first-degree injury consists of only mild stretching of the ligament. There is no looseness. A second-degree LCL is a partial tear of the ligament. In a third-degree injury, the ligament is completely ruptured, and the joint is unstable.
What are the symptoms?
What are the prevention of the injury? Many LCL injuries cannot be prevented. However, to lessen the risk of injury, a person should be in good physical shape before engaging in sporting activities. Sports safety guidelines should be followed for adults, adolescents and children. Proper stretching exercises should be done prior to athletic activity.
What are the treatment? The treatment for LCL injuries depends on the severity of the problem. The kind of activities a person is likely to do in the future is also taken into account. RICE, which stands for rest, ice, compression with an ace bandage, and elevation of the leg, is the standard initial treatment. Medicine, such as nonsteroidal anti-inflammatory drugs (NSAIDs), can be used for pain. Crutches can be helpful until motion and strength in the joint have improved. Occasionally, a brace is used for a few days to immobilize the knee.
The person also needs to do knee exercises to regain flexibility in the joint and strength in the thigh muscle. Physical therapy is sometimes needed to help with this. The individual should also take care to avoid reinjuring the joint before it has completely healed. Surgery may be needed in severe cases where the ligament has been torn and the knee is unstable.
What are the symptoms?
- Discomfort on the outside of the knee when tension is applied
- Pain and swelling on the outside of the knee
- When the area over the affected ligament is touched
- Weakness of the knee
What are the prevention of the injury? Many LCL injuries cannot be prevented. However, to lessen the risk of injury, a person should be in good physical shape before engaging in sporting activities. Sports safety guidelines should be followed for adults, adolescents and children. Proper stretching exercises should be done prior to athletic activity.
What are the treatment? The treatment for LCL injuries depends on the severity of the problem. The kind of activities a person is likely to do in the future is also taken into account. RICE, which stands for rest, ice, compression with an ace bandage, and elevation of the leg, is the standard initial treatment. Medicine, such as nonsteroidal anti-inflammatory drugs (NSAIDs), can be used for pain. Crutches can be helpful until motion and strength in the joint have improved. Occasionally, a brace is used for a few days to immobilize the knee.
The person also needs to do knee exercises to regain flexibility in the joint and strength in the thigh muscle. Physical therapy is sometimes needed to help with this. The individual should also take care to avoid reinjuring the joint before it has completely healed. Surgery may be needed in severe cases where the ligament has been torn and the knee is unstable.
Meniscus Injuries
What are the prevention of the injury? Many LCL injuries cannot be prevented. However, to lessen the risk of injury, a person should be in good physical shape before engaging in sporting activities. Sports safety guidelines should be followed for adults, adolescents and children. Proper stretching exercises should be done prior to athletic activity.
What are the treatment? The treatment for LCL injuries depends on the severity of the problem. The kind of activities a person is likely to do in the future is also taken into account. RICE, which stands for rest, ice, compression with an ace bandage, and elevation of the leg, is the standard initial treatment. Medicine, such as nonsteroidal anti-inflammatory drugs (NSAIDs), can be used for pain. Crutches can be helpful until motion and strength in the joint have improved. Occasionally, a brace is used for a few days to immobilize the knee.
The person also needs to do knee exercises to regain flexibility in the joint and strength in the thigh muscle. Physical therapy is sometimes needed to help with this. The individual should also take care to avoid reinjuring the joint before it has completely healed. Surgery may be needed in severe cases where the ligament has been torn and the knee is unstable.
What are the treatment? The treatment for LCL injuries depends on the severity of the problem. The kind of activities a person is likely to do in the future is also taken into account. RICE, which stands for rest, ice, compression with an ace bandage, and elevation of the leg, is the standard initial treatment. Medicine, such as nonsteroidal anti-inflammatory drugs (NSAIDs), can be used for pain. Crutches can be helpful until motion and strength in the joint have improved. Occasionally, a brace is used for a few days to immobilize the knee.
The person also needs to do knee exercises to regain flexibility in the joint and strength in the thigh muscle. Physical therapy is sometimes needed to help with this. The individual should also take care to avoid reinjuring the joint before it has completely healed. Surgery may be needed in severe cases where the ligament has been torn and the knee is unstable.
Iliobtibial Band Syndrome
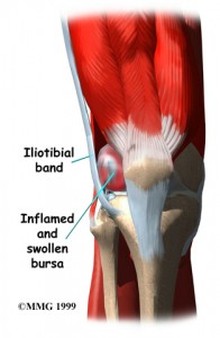
What is Iliobtibial Band Syndrome? The iliotibial band is a strong, thick band of fibrous tissue that runs along the outside of the leg. The IT band starts at the hip and runs along the outer thigh and attaches on the outside edge of the shin bone just below the knee joint. The band works with the thigh muscles to provide stability to the outside of the knee joint during movement.
What are the causes?
What are the causes?
- Overuse
- Increase the intensitivity too quickly
- Returning from injury too soon
- Treatment of MCL tear
- Foam Roller Myofacial Release
- Anti-Inflammatory Medication
- Rest and recover
Plica Syndrome
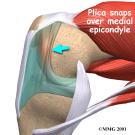
What is Plica Syndrome? This inflammation is typically caused by the plica being caught on the femur, or pinched between the femur and the patella. The most common location of plica tissue is along the medial (inside) side of the knee. The plica can tether the patella to the femur, be located between the femur and patella, or be located along the femoral condyle. If the plicae tethers the patella to the femoral condyle, the symptoms may cause it to be mistaken for Patello-femoral Syndrome. Because of this similarity in symptoms, Plica Syndrome is frequently misdiagnosed as Patello-femoral Syndrome. Diagnosis is often complicated by the thin structures of plicae, fenestrated septum or unfenestrated septum all being too fine to resolve well even in MRI.
The plica themselves are remnants of the fetal stage of development where the knee is divided into three compartments. The plica normally diminish in size during the second trimester of fetal development, as the three compartments develop into the synovial capsule. In adults, they normally exist as sleeves of tissue called synovial folds. The plica are usually harmless and unobtrusive; Plica Syndrome only occurs when the synovial capsule becomes irritated, which thickens the plica themselves (making them prone to irritation/inflammation, or being caught on the femur).
What are the causes?
The plica themselves are remnants of the fetal stage of development where the knee is divided into three compartments. The plica normally diminish in size during the second trimester of fetal development, as the three compartments develop into the synovial capsule. In adults, they normally exist as sleeves of tissue called synovial folds. The plica are usually harmless and unobtrusive; Plica Syndrome only occurs when the synovial capsule becomes irritated, which thickens the plica themselves (making them prone to irritation/inflammation, or being caught on the femur).
What are the causes?
- Overuse Injury
- Injury to the joint
|
Knee Dislocation
What is Knee Dislocation? A knee dislocation occurs when the bones that form your knee are out of place.
The bones of your calf (the tibia and fibula) get moved compared to the bone of your thigh (femur). The bones of your knee are held together by strong bands of tissue, called ligaments. For a knee dislocation to happen, these bands have to tear.
What are the symptoms? Specifically, there will be a large amount of pain in the knee. Sometimes, there will be no feeling below the knee. If the knee relocates, it will become swollen. You may not be able to feel a pulse (your heartbeat) in your foot.
What are the causes? Knee dislocations are rare. They usually happen only after major trauma, including falls, car crashes, and other high-speed injuries.
The bones of your calf (the tibia and fibula) get moved compared to the bone of your thigh (femur). The bones of your knee are held together by strong bands of tissue, called ligaments. For a knee dislocation to happen, these bands have to tear.
What are the symptoms? Specifically, there will be a large amount of pain in the knee. Sometimes, there will be no feeling below the knee. If the knee relocates, it will become swollen. You may not be able to feel a pulse (your heartbeat) in your foot.
What are the causes? Knee dislocations are rare. They usually happen only after major trauma, including falls, car crashes, and other high-speed injuries.
- If the knee is dislocated, it will look deformed. The usual straight line of your leg will be crooked.
- Sometimes, knee dislocations relocate (go back into place) on their own. In this case, the knee will be very swollen and painful.
- Relocation of your knee
- Immobilization
- Surgery
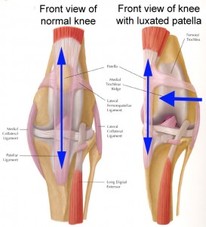
Unstable Kneecap
What is Unstable Kneecap? Unstable Knee cap happens when the patella of your knee start to move out of its original place.
What are the symptoms?
Treatment of MCL tear
What are the symptoms?
- Stiffness
- Swelling
- Cracking sound during movement
- Kneecap slips off to the side
- Pain in the front of the knee that increase with activity
Treatment of MCL tear
- Relocation of your knee
- Immobilization
- Surgery